
Let’s be real for a second. If you’ve gone looking into peptides at all, you’ve probably run across ipamorelin, and you’ve probably run across somebody selling it like it’s a settled deal. It is not. Ipamorelin is not an FDA-approved drug, and the human evidence behind it is a lot thinner than the marketing lets on. There’s no white coat standing at the top of this piece, and that’s on purpose. What you get instead is a paper trail, three primary sources you can go read yourself [1][2][3], because trust ought to live in the documents, not in whoever’s name is signed at the bottom.
Here’s the shape of the story, and I think it’s worth telling this way because it’s the honest one: ipamorelin is about as cleanly built as a growth hormone secretagogue gets. It performed exactly like it was supposed to in the lab. Then it went into an actual randomized trial in actual human beings, the one test that was supposed to prove it out, and it came up short. The company behind it moved on. That’s not a knock. That’s just what happened, and it’s the frame this whole article hangs on.
What the thing actually is
Ipamorelin is a small, synthetic chain of five amino acids (Aib-His-D-2-Nal-D-Phe-Lys-NH2, if you want the exact arrangement). It sits in a class called growth hormone secretagogues. It doesn’t hand your body growth hormone. It knocks on the door of your pituitary gland and asks it to release a pulse of the stuff on its own, by working the ghrelin receptor, the GHS-R1a, same receptor your hunger hormone uses. It’s given as a subcutaneous shot, and folks often pair it with a peptide called CJC-1295. That combo gets its own coverage elsewhere in this series. Here we’re keeping the lens on ipamorelin by itself.
The thing that made it interesting in the first place is selectivity. Earlier secretagogues like GHRP-6 and GHRP-2 do bump growth hormone up, but they drag cortisol, ACTH, and prolactin along for the ride, which is exactly what somebody chasing recovery or better body composition doesn’t want. Ipamorelin was built to skip that side trip, and the early research backed that up. That’s a real pharmacological trait. It’s not just a line copywriters like.
Where that reputation comes from, and where it stops
The selectivity claim traces back to one well-known 1998 study in the European Journal of Endocrinology, the paper that introduced the compound. Researchers found ipamorelin released growth hormone about as well as GHRP-6 in rat pituitary cells and in pigs, but unlike GHRP-6 and GHRP-2, it didn’t push ACTH or cortisol up meaningfully beyond what plain growth hormone releasing hormone stimulation produced, even at high doses [1]. That’s a solid, specific, repeatable finding, and it’s why people took ipamorelin seriously to begin with.
Here’s the part that matters just as much: that whole study happened in rat cells, sedated rats, and pigs. No people. The selectivity is real, and it’s held up over time, but it was shown in animals. A result like that earns a compound the right to be tested in humans. It doesn’t tell you what happens once a human being takes it.
The trial nobody puts on the label
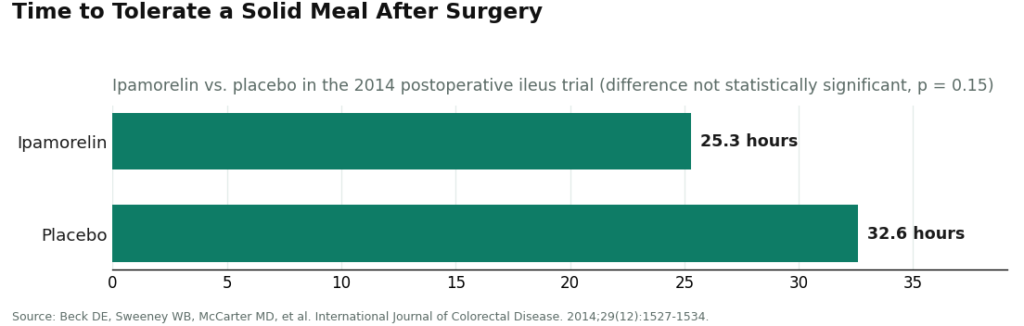
This is the fact that gets buried, and it shouldn’t. Ipamorelin actually made it into human trials, properly designed ones, and the result was a miss. The biggest published human study put ipamorelin up against a real clinical problem: postoperative ileus, that stretch after abdominal surgery when your bowels shut down for a while. It was a prospective, randomized, double-blind, placebo-controlled trial, published in the International Journal of Colorectal Disease in 2014, 117 patients enrolled, 114 in the final analysis [2].
Let’s put the numbers right out on the table, because they’re the whole point. Patients on ipamorelin got back to eating a solid meal at a median of 25.3 hours after surgery. Placebo patients got there at 32.6 hours. Sounds like a win at a glance. Run the statistics, though, and the difference wasn’t significant, p equals 0.15, and the trial didn’t find meaningful differences from placebo on its other measures either. What it did confirm was that ipamorelin was well tolerated at the dose they used [2].
So say it plain: the best human trial ipamorelin ever had showed it was safe and it didn’t work for what it was tested on. That’s a big reason nobody pushed it further as an actual drug. And here’s the angle worth sitting with, because it’s the whole ballgame, really: that surgical trial is the strongest human evidence ipamorelin has, period. Everything the market sells it for, fat loss, recovery, anti-aging, rests on evidence that’s even lighter than the study that already came back negative. A compound that missed its mark in a controlled hospital setting isn’t quietly winning somewhere else with no trial at all.
What the animal data actually buys you
The benefits you’ll hear cited most, bone, muscle, recovery, all trace back to animal research, and you should weigh them at exactly that level. A 2001 study in Growth Hormone and IGF Research found ipamorelin counteracted glucocorticoid-related bone loss in adult rats, with periosteal bone formation running roughly four times higher when ipamorelin was given alongside the glucocorticoid, compared to the glucocorticoid alone [3]. That’s a genuinely interesting result. It’s also rats.
Animal studies like this are how a compound earns a shot at human trials. They’re not proof the same thing happens in people, at the same size, without unwanted long-term baggage. The controlled human trials that would actually confirm a bone, muscle, or recovery benefit mostly haven’t been run. So the fair way to say it is: ipamorelin does real things to growth hormone signaling, and it’s shown some promising tissue effects in animals, but the payoff people actually want, the human one, is still unproven.
About those dosing charts you keep seeing
You’ll find confident-looking dosing charts all over, microgram doses, once or twice a day, often timed around sleep or training, sometimes run in cycles. Worth being straight about where those numbers came from: community and clinical convention, not human trials proving they work for body composition or anti-aging, because those trials don’t exist. The only controlled human dosing on record is that 2014 surgical trial, run for up to seven days in a hospital under monitoring, and it didn’t hit its endpoint [2]. That’s a different world from months of self-injecting at home.
Bottom line here: there’s no dose of ipamorelin backed by human outcome data for the reasons people are buying it. Any protocol you find is a starting convention somebody made up, not a prescription earned through evidence, and figuring out dosing is exactly the kind of call that belongs to a licensed clinician who knows your history and your medications, not a chart lifted off a forum. This article won’t hand you one either.
Safety: fine for a week, foggy after that
The honest safety picture is short-term reassurance and long-term fog. That 2014 trial showed good tolerability over up to seven days in surgical patients under hospital watch [2]. That’s real, but it’s narrow. A week in a hospital bed isn’t the same as months or years of self-injecting at home. The mild stuff that shows up, water retention, headache, lightheadedness, injection site irritation, tracks with what you’d expect from secretagogues generally. What nobody’s really nailed down in humans is what happens when you keep stimulating growth hormone release chronically in an otherwise healthy adult over a long stretch. That’s not a reason to panic. It’s a reason to go slow and stay supervised, and no certificate of analysis on a vial is going to fill that gap for you.
The rulebook, briefly
Two things round this out. First, ipamorelin is not FDA-approved, and its place in pharmacy compounding is contested, not settled. The FDA’s Pharmacy Compounding Advisory Committee, which weighs in on what bulk substances pharmacies can legally use under section 503A, looked at ipamorelin and voted against putting it on that list [4], and the committee’s still working through peptide nominations into 2026 [5]. So being able to buy it through a compounding pharmacy is not the same thing as the FDA giving it a nod. If you hear that ipamorelin got “reinstated” or “approved” for compounding recently, go check the FDA’s own record before you believe it. This ground shifts.
Second, ipamorelin is named right there on the WADA 2026 Prohibited List, under S2, peptide hormones, growth factors, and mimetics, as a growth hormone secretagogue and ghrelin-receptor agonist [6]. It’s banned in sport, full stop, and a “research use only” sticker on a vial does not protect a tested athlete from a single thing. If you compete in a tested sport, treat this and anything like it as off the table, and check the current list before you go anywhere near it.
Where oversight actually earns its keep
None of what’s above changes just because somebody decides to use ipamorelin anyway. But how that decision gets made can change a whole lot. Most of what you’ll stumble into when you search this stuff is the gray-market route: a freeze-dried vial in bubble wrap, stamped not for human use, run through a checkout that never once asked who you were or what you’re taking it for. A supervised path looks different, and it maps right onto the exact gaps this whole article has walked through: a licensed clinician looks at your history and your current meds, decides whether a growth hormone secretagogue makes any sense for you at all, writes a prescription if it does, and a licensed pharmacy compounds and dispenses it, with someone to follow up with afterward. Of the setups built that way, FormBlends is the clearest example of putting the clinician at the front door instead of the checkout page, and a supervised program like HealthRX runs in that same regulated lane behind it. None of that makes ipamorelin proven. What it does is put the accountability and medical judgment back into a process a mailed research vial was built to skip.
Let’s not soften this part either: compounded medications are not FDA-approved finished drug products. The FDA doesn’t review them for safety, effectiveness, or quality the way it reviews the drugs on your pharmacy shelf. What a compliant, supervised setup adds is the clinical screening and follow-up wrapped around the compounding, which is exactly the layer a research vial mailed to your door never claimed to have.
Where I land on this
Ipamorelin is a real, cleverly built molecule with a selectivity edge that’s held up in animal studies, one neutral-but-safe human trial, some promising rodent findings on bone, and not much long-term human safety data to go on. It is not a proven human treatment for the recovery, body composition, or anti-aging claims it gets sold under. You’ve got to hold both halves in your head at once, the strong mechanism and the thin clinical record, because the marketing’s only going to give you the first half, loud and clear, and go quiet on the second.
Questions people actually ask
Has ipamorelin ever actually been tested on people?
Yes, and this is the part worth remembering. The biggest published human study was a properly randomized, double-blind, placebo-controlled trial testing ipamorelin against postoperative ileus, published in 2014 with 117 patients enrolled [2]. It was well tolerated, but it missed its primary endpoint: time to a solid meal came in at a median of 25.3 hours on ipamorelin versus 32.6 hours on placebo, and that gap wasn’t statistically significant (p = 0.15). That negative result is a big part of why the drug never went further.
What’s this “selective” thing everybody talks about?
It means ipamorelin sparks a growth hormone pulse without dragging ACTH, cortisol, or prolactin up along with it, the way older peptides like GHRP-6 and GHRP-2 do. The 1998 study that introduced the compound showed it matched GHRP-6 for potency while leaving ACTH and cortisol close to baseline, even at high doses [1]. Just remember, that clean profile was shown in rat cells and pigs, not people.
Are the bone, muscle, and recovery benefits real?
They come almost entirely out of animal research, so weigh them that way. A 2001 rat study found ipamorelin countered glucocorticoid-related bone loss, with periosteal bone formation running about four times higher than glucocorticoid alone [3], a genuinely interesting rodent result. What’s missing is the human trial work that would confirm the same thing happens in people, at a useful level, without long-term downsides.
Is there a real, evidence-backed dose for body composition or anti-aging use?
No. The dosing charts floating around online are convention, not something proven out in human trials for those purposes, because those trials haven’t happened. The only controlled human dosing we’ve got is that 2014 surgical trial, run for up to a week under hospital supervision [2], which is a far cry from months of self-injecting. Dose decisions belong with a licensed clinician who knows your full picture.
Can you legally buy it, and can athletes use it?
Ipamorelin isn’t FDA-approved, and the FDA’s own compounding advisory committee voted against adding it to the approved bulk substances list, with peptide review still ongoing into 2026 [4][5]. In sport, it’s specifically named on the WADA 2026 Prohibited List under S2 [6], so a “research use only” sticker offers zero protection to a tested athlete. Getting it through a compounding pharmacy isn’t the same as an FDA green light.
What’s it actually doing inside your body?
It latches onto ghrelin receptors in your pituitary and triggers a pulse of growth hormone release, following your body’s own natural rhythm instead of just flooding the system. That’s why it caught researchers’ attention. What that pulse actually delivers for a healthy adult, whether it turns into real fat loss, muscle gain, or faster recovery, hasn’t been nailed down in controlled human trials.
Does stacking CJC-1295 with ipamorelin actually beat either one alone?
The pairing is popular because the two hit different spots in the growth hormone pathway. CJC-1295 stretches out the signal from the hypothalamus while ipamorelin works the pituitary directly, so the theory says together you get a bigger, longer pulse. That’s a reasonable idea on paper, but there’s no human clinical evidence yet showing the combo delivers real body composition or performance results. Plausible, not proven.
Is that combination safe?
There’s no large-scale human safety data on the combo, so anybody claiming otherwise is guessing. Ipamorelin by itself showed a cleaner side-effect profile than the older secretagogues in animal and early human work, less cortisol and prolactin spiking, but that’s a relative comparison at research doses, not a stamp of approval. Sourcing is a big deal here too. Peptides bought through unregulated research-chemical channels carry real contamination and dosing risk that a physician-supervised compounding pharmacy like FormBlends is built to guard against.
How’s it different from actual growth hormone injections?
Ipamorelin is a five-amino-acid peptide that tells your pituitary to release its own growth hormone, rather than putting exogenous GH straight into your system. That matters because your pituitary still applies its own natural brakes, part of why it was considered a safer research candidate than direct HGH. Both paths, though, remain either prescription-only or outright unapproved depending on where you live, and neither one has solid human proof behind the anti-aging or body composition claims most buyers are chasing.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998;139(5):552-561. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Beck DE, Sweeney WB, McCarter MD; Ipamorelin 201 Study Group. Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease. 2014;29(12):1527-1534. https://link.springer.com/article/10.1007/s00384-014-2030-8
- Svensson J, Lall S, Dickson SL, et al. The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats. Growth Hormone and IGF Research. 2001;11(5):266-272.
- U.S. Food and Drug Administration. Pharmacy Compounding Advisory Committee briefing materials and votes on bulk drug substances nominated under section 503A (ipamorelin not recommended for inclusion). 2024.
- U.S. Food and Drug Administration. Meeting of the Pharmacy Compounding Advisory Committee, July 23-24, 2026 (ongoing review of nominated peptide bulk drug substances).
- World Anti-Doping Agency. The 2026 Prohibited List, Section S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics. In force 1 January 2026.
Written by Hugo Rossi, analytics writer. Reporting from the sources cited above. Last reviewed January 2026.
General educational content. Speak with a licensed professional before changing your routine.




